Regulations in Toxicology
FAERS Safety Signals in 2025: What Medical Toxicologists Should Watch
Omid Mehrpour
Post on 24 Dec 2025 . 8 min read.
Omid Mehrpour
Post on 24 Dec 2025 . 8 min read.

By 2025, the landscape of drug safety surveillance in the United States is shifting in important ways. The FDA Adverse Event Reporting System (FAERS) is moving toward near real-time data, and new safety signals and regulatory communications are emerging for very common drugs, including acetaminophen and GLP-1 receptor agonists.[1–5]
If you already know roughly what is FAERS and why it matters in medical toxicology, the practical question becomes:
In 2025, which FAERS signals and FDA Drug Safety Communications actually matter for medical toxicology?
This blog highlights the most relevant FAERS potential signals (Q2 2025) and 2025 FDA Drug Safety Communications (DSCs) that intersect with overdose, serious toxicity, or poisoning-like presentations, and translates them into clinical and toxicology takeaways.
The most recent FAERS “Potential Signals of Serious Risks/New Safety Information” list, covering April–June 2025, was posted on September 30, 2025.[1] It summarizes drug–event pairs that have triggered signal detection thresholds and are under FDA evaluation.
Several of these signals are directly relevant to emergency medicine, intensive care, and poison center practice.
For the first time, FAERS lists a potential signal for anaphylactic reactions associated with:
Acetaminophen-containing products.[1]
We traditionally think of acetaminophen (APAP) as a dose-dependent hepatotoxin and a classic overdose agent. This signal suggests there may also be a rare but serious hypersensitivity component.
If you’re managing a suspected or confirmed acetaminophen (APAP) poisoning case, using RumackCalc and ApapTox can make your work faster and safer. RumackCalc helps you quickly interpret the Rumack–Matthew nomogram and choose the right NAC plan. At the same time, ApapTox adds decision support for delayed or repeated ingestions using lab-guided risk assessment to sharpen both diagnosis and treatment.
Toxicology implications:
In cases of sudden anaphylaxis/shock where the usual suspects (β-lactams, contrast, latex, foods) do not fully explain the timing, recent APAP exposure—especially IV acetaminophen or multi-ingredient OTC products—should be included in the history and the differential.
This does not mean APAP is now a common cause of anaphylaxis. It can be among the plausible triggers in selected cases.
FAERS has flagged a potential signal for:
GLP-1 receptor agonists (e.g., semaglutide, liraglutide)
→ Intestinal obstruction / fecal impaction.[1]
It builds on existing worries that GLP-1 drugs don’t just cause mild nausea —in rare cases, they can slow the gut so much that patients develop a real bowel obstruction.
Toxicology implications:
A patient on a GLP-1 drug who has belly pain, ongoing vomiting, and no gas or stool should not be brushed off as having “just Ozempic nausea.”
You should maintain a low threshold for imaging. In high-risk patients or when symptoms are disproportionate, early surgical consultation is recommended to rule out mechanical obstruction.
The association between:
SGLT2 inhibitors (e.g., canagliflozin, empagliflozin)
→ Fournier’s gangrene (necrotizing perineal infection)
remains prominent in FAERS signals and product labeling.[1]
Toxicology implications:
Any perineal pain, swelling, erythema, or systemic toxicity in an SGLT2-treated patient should immediately raise suspicion for necrotizing soft-tissue infection, specifically Fournier’s gangrene.
This is not classic “poisoning,” but it is a catastrophic, drug-associated condition squarely within the purview of med tox and ICU consults.
Related Topic: Guidelines for Ozempic (Semaglutide) Toxicity: Epidemiology, Management, and Safety
FAERS lists a potential signal for:
Topiramate-containing products → Hypersensitivity reactions.[1]
Anticonvulsant hypersensitivity syndrome (AHS) is usually linked to aromatic AEDs (e.g., carbamazepine, phenytoin). Topiramate is non-aromatic, but:
Toxicology implications:
In a patient on a multi-AED regimen who presents with rash, fever, eosinophilia, and multi-organ involvement, topiramate should now be considered among the possible culprits in addition to the usual suspects.
This matters for dechallenge/rechallenge decisions and for how you advise teams about which drug(s) to discontinue.
The FAERS potential signal list also includes:
Barium sulfate products → Hypersensitivity/anaphylactic reactions
Several PET imaging agents (e.g., flutemetamol F-18, Vizamyl) → Anaphylaxis/severe hypersensitivity, with some labels already updated.[1]
Toxicology implications:
When a patient collapses or becomes hemodynamically unstable after a radiologic procedure, it is worth remembering that:
Oral barium suspensions
and PET tracers
It can sometimes cause systemic hypersensitivity, not only to iodinated IV contrast.
For ED/ICU and tox, these agents belong in the differential for post-procedure anaphylaxis.
Related Topic: Clinical features and management strategies of acute soluble barium poisoning: a review of case reports.

Beyond FAERS signal tables, the FDA issues Drug Safety Communications (DSCs) for risks that are sufficiently serious and supported to warrant explicit public guidance.
In 2025, two DSCs stand out for toxicology:
A class-wide labeling update for all opioid pain medicines
A scopolamine patch warning for heat-related toxicity
On July 31, 2025, the FDA issued a DSC requiring manufacturers of all opioid pain medications to update their prescribing information.[2,6]
Key points:
Long-term opioid use is now more explicitly framed as carrying:
Misuse and addiction risk
Fatal and nonfatal overdose risk
Serious harms across the entire treatment course[2,6]
Labels must be clearer:
Highlight these risks to prescribers
Encourage discussions about overdose reversal agents (e.g., naloxone, nalmefene)
Emphasize careful consideration of dose and duration
Toxicology implications:
Overdose is reframed not just as a “street fentanyl” problem, but as a predictable hazard of long-term opioid therapy.
For poison centers and med tox services, this DSC:
Strengthens arguments for naloxone co-prescribing
Supports intervention in cases of clearly risky chronic regimens
Provides official language you can quote in guidelines, consult notes, and education.
Related Blog: Fentanyl + Xylazine (‘Tranq’): Why Naloxone Alone Isn’t Enough
In mid-2025, the FDA added a warning that the Transderm Scōp® (scopolamine transdermal system) can:[3]
Reduce the body’s ability to dissipate heat
Lead to heat-related complications (including hyperthermia and confusion)
Result in hospitalization or death, particularly in:
Children and adolescents
Older adults
Patients exposed to hot environments (travel, outdoor activities, cruises)
Toxicology implications:
This is essentially a real-world description of an anticholinergic toxidrome + heat stress:
Signs can include:
Delirium or agitation
Elevated core temperature
Tachycardia
Dry, flushed skin
In an older traveler or a child with confusion, hyperthermia, and a visible scopolamine patch in a hot setting, you should treat the situation as anticholinergic toxicity in the setting of heat, not just “heat stroke” or dehydration.

All FAERS signals and DSCs depend on someone actually reporting adverse events.
That “someone” is often you, via MedWatch:
MedWatch is the FDA’s safety information and adverse event reporting program, used by clinicians, pharmacists, and patients.[3,4]
Reports submitted through MedWatch feed directly into the FAERS database, where they can contribute to signal detection and ultimately inform label changes and DSCs.
Why this matters to toxicologists:
Severe or unusual events you see — overdose patterns, hypersensitivity, new toxidromes — will not contribute to national signal detection unless somebody reports them.
Under-reporting is a major limitation of FAERS.[7] When toxicologists and poison centers take the time to file MedWatch reports, they directly influence the likelihood and timing of a safety signal being recognized.
Acute anaphylaxis/shock:
In the right context, acetaminophen-containing products should now appear in the list of possible triggers.[1]
Severe GI complaints in GLP-1 users:
Think mechanical obstruction, not just “nausea from a weight-loss drug.”[1]
Perineal sepsis in SGLT2 users:
Maintain a low threshold to suspect Fournier’s gangrene and involve surgery early.[1]
Confusion + hyperthermia + scopolamine patch + heat exposure:
Consider an anticholinergic heat toxidrome, not only infectious or environmental heat stroke.[3]
When you:
Advocate for naloxone co-prescribing
Argue for the de-escalation of long-term opioids
Teach about GLP-1 or SGLT2 serious adverse events
Explain anticholinergic + heat interactions
…you can reference:
The July 31, 2025, opioid DSC for long-term overdose and addiction risk[2,6]
The Transderm Scōp DSC for heat-related toxicity[3]
The Q2 2025 FAERS signal list for APAP anaphylaxis and GLP-1/SGLT2 events[1]
That framing turns “my tox opinion” into “my tox opinion, aligned with FDA’s current safety view.”
Remember:
FAERS is:
Excellent for therapeutic drug safety signals
Poor for illicit drug trends (fentanyl analogues, nitazenes, xylazine, “space oil” etomidate)
Not suitable for estimating incidence (no denominator, lots of reporting bias)[7]
Your core toxicology data streams are still:
NPDS and poison center databases
Medical examiner and forensic toxicology
EHR/claims for denominators and outcomes
The optimal 2025 posture is:
Use FAERS as a regulatory lens on drug toxicity that sits alongside your clinical and surveillance data — not instead of them.
For medical toxicologists, four 2025 safety themes are worth carrying into 2026:
Acetaminophen beyond the liver
Rare but serious anaphylactic reactions are now flagged as a potential FAERS signal.[1]
GLP-1 and SGLT2 serious complications
Obstruction and Fournier’s gangrene are real, serious risks, not mere “nuisance side effects.”[1]
Opioid class-wide DSC
Long-term opioid prescribing is explicitly framed as carrying addiction and overdose risk, with a push toward naloxone co-prescribing.[2,6]
Transderm Scōp and heat
Anticholinergic toxicity in the context of heat exposure is now formally recognized in labeling, especially for children and older adults.[3]
These themes are strong enough to justify updating protocols, teaching materials, and consult templates for the coming year.
© All copyright of this material is absolute to Medical toxicology
Dr. Omid Mehrpour (MD, FACMT) is a senior medical toxicologist and physician-scientist with over 15 years of clinical and academic experience in emergency medicine and toxicology. He founded Medical Toxicology LLC in Arizona and created several AI-powered tools designed to advance poisoning diagnosis, clinical decision-making, and public health education. Dr. Mehrpour has authored over 250 peer-reviewed publications and is ranked among the top 2% of scientists worldwide. He serves as an associate editor for several leading toxicology journals and holds multiple U.S. patents for AI-based diagnostic systems in toxicology. His work brings together cutting-edge research, digital innovation, and global health advocacy to transform the future of medical toxicology.
U.S. Food and Drug Administration. Potential Signals of Serious Risks/New Safety Information Identified from the FDA Adverse Event Reporting System (FAERS): April–June 2025 [Internet]. Silver Spring (MD): FDA; 2025 Sep 30 [cited 2025 Dec 17]. Available from: https://www.fda.gov/drugs/fdas-adverse-event-reporting-system-faers/potential-signals-serious-risksnew-safety-information-identified-fda-adverse-event-reporting-system
U.S. Food and Drug Administration. FDA is requiring opioid pain medicine manufacturers to update prescribing information regarding long-term use (Drug Safety Communication) [Internet]. Silver Spring (MD): FDA; 2025 Jul 31 [cited 2025 Dec 17]. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-requiring-opioid-pain-medicine-manufacturers-update-prescribing-information-regarding-long-term
U.S. Food and Drug Administration. FDA adds warning about serious risk of heat-related complications with antinausea patch Transderm Scōp (scopolamine transdermal system) [Internet]. Silver Spring (MD): FDA; 2025 Jun 18 [cited 2025 Dec 17]. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-adds-warning-about-serious-risk-heat-related-complications-antinausea-patch-transderm-scop
U.S. Food and Drug Administration. MedWatch: The FDA Safety Information and Adverse Event Reporting Program [Internet]. Silver Spring (MD): FDA; 2025 Oct 15 [cited 2025 Dec 17]. Available from: https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program
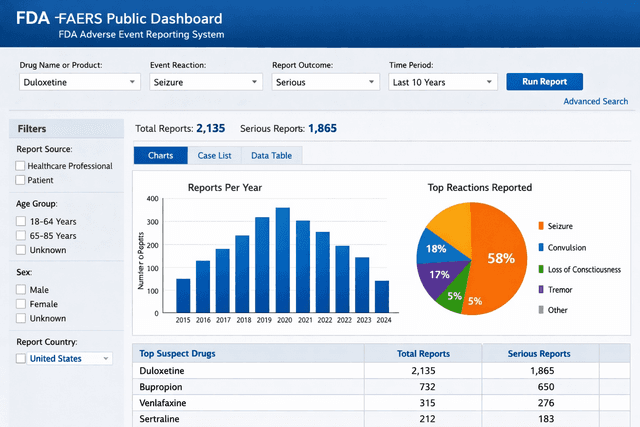
U.S. Food and Drug Administration. FDA Adverse Event Reporting System (FAERS) Public Dashboard [Internet]. Silver Spring (MD): FDA; 2025 [cited 2025 Dec 17]. Available from: https://www.fda.gov/drugs/fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard
U.S. Food and Drug Administration. Drug Safety Communications [Internet]. Silver Spring (MD): FDA; 2025 [cited 2025 Dec 17]. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/drug-safety-communications
Potter E, et al. FDA Adverse Event Reporting System (FAERS) essentials: a practical guide. Clin Pharmacol Ther. 2025;118(3):567–582. doi:10.1002/cpt.3701.