DEA Begins Schedule I Process for Concentrated 7-OH as Poison-Center Reports Rise
post on 15 Jul 2026
post on 15 Jul 2026
DEA Begins Schedule I Process for Concentrated 7-OH as Poison-Center Reports Rise
US regulators have begun the process of temporarily controlling concentrated 7-hydroxymitragynine products as poison centers report a sharp rise in exposures. The action is not yet in force and is not a blanket federal ban on natural kratom leaf.
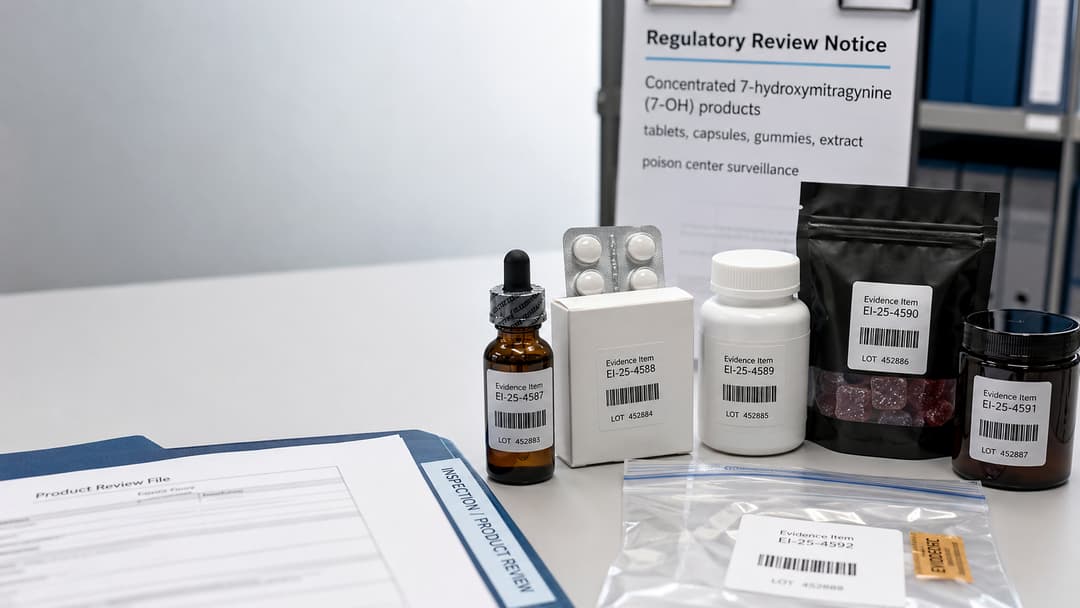
The US Drug Enforcement Administration (DEA) announced on 1 July 2026 that it intends to place concentrated 7-hydroxymitragynine, commonly called 7-OH, and three related substances temporarily in Schedule I of the Controlled Substances Act. The Food and Drug Administration (FDA) updated its public-health information on 13 July to explain the action and distinguish the targeted products from botanical kratom containing only naturally occurring trace amounts of 7-OH. A B
Formal notices were published in the Federal Register on 6 July. One covers 7-OH above a specified concentration or quantity threshold. A second covers mitragynine pseudoindoxyl, MGM-15 and MGM-16, substances produced through chemical modification of mitragynine or 7-OH. C D
As of 15 July, the substances covered by the notices have not yet been temporarily placed in Schedule I. The temporary order for 7-OH cannot be issued before 5 August and would take effect only when a final order is published in the Federal Register. It would initially remain in force for two years and could be extended for one additional year while permanent scheduling proceedings continue. C
It is therefore inaccurate to report that 7-OH has already been federally banned or that all kratom products are becoming Schedule I substances.
The proposed threshold covers botanical Mitragyna speciosa material containing more than 0.050% 7-OH by dry weight.
For synthetic or processed products—including extracts, concentrates, edibles and pressed pills—the notice applies when 7-OH exceeds 0.050% by weight, volume or an applicable weight-to-volume measurement, or when an article contains more than 1 milligram of 7-OH. Relevant isomers, esters, ethers and salts are also included when chemically possible. C
The threshold is not beyond review. The Department of Health and Human Services has requested scientific information on whether it accurately identifies products that pose an imminent public-safety hazard, with comments accepted through 31 July. E
7-OH occurs naturally in small amounts in the kratom plant. The current federal action is aimed primarily at synthesised, chemically enhanced and highly concentrated products rather than botanical material that remains below the proposed threshold.
Some commercial products contain far more 7-OH than would normally be expected in unprocessed leaf and may be sold as tablets, gummies, capsules, powders, strips or concentrated extracts. The FDA says there are no approved drugs containing kratom or 7-OH for pain, opioid withdrawal, anxiety, depression or any other medical indication. A
The shift from traditional plant preparations to concentrated or chemically altered products reflects the wider toxicology problem discussed in Inside the Synthetic Drug Surge: Why 2025's New Threats Are Different.
America’s Poison Centers recorded 3,803 reports involving kratom or kratom derivatives during 2025. Between 1 January and 30 June 2026, centers had already received 3,190 reports. If that pace continued for the full year, it would represent a projected 67.8% increase compared with 2025. F
Reports specifically coded as 7-OH increased from 593 during all of 2025 to 901 during the first six months of 2026. The average monthly count in 2026 was 102% higher than during the final six months of 2025.
Among reports identifying 7-OH as the only substance involved, 38.8% were associated with serious health problems, 63.8% received treatment at a healthcare facility and 20.5% resulted in hospital admission. F
These are poison-center exposure reports, not a direct measure of national use or incidence. They also do not prove that 7-OH alone caused every reported effect. Increased awareness and the introduction of a specific 7-OH coding category during 2025 may have influenced reporting.
A broader explanation of how poison-center consultations become public-health signals is available in The Role of Poison Center Calls: Managing Poisoning Cases from Emergency Calls to Critical Decisions.
A 2026 analysis in the Morbidity and Mortality Weekly Report examined 14,449 kratom-related reports submitted to US poison centers between 2015 and 2025. Reports rose from 258 in 2015 to 3,434 in 2025. Multiple-substance cases were more likely than single-substance reports to involve hospitalisation, serious medical effects or death. Of 233 kratom-associated deaths, 184 involved multiple substances, commonly opioids, benzodiazepines, stimulants or alcohol. G
A separate 2026 study in The American Journal of Emergency Medicine reviewed 13,194 reports from January 2016 through July 2025. Ten per cent involved major effects and 1.6% involved death, with most deaths occurring in polysubstance cases. The study found a marked increase in reports during 2025, although the overall distribution of clinical outcomes remained broadly similar. H
Neither study proves that concentrated 7-OH caused the entire increase. Product identity and concentration were not consistently verified, and the word “kratom” may refer to botanical leaf, extracts, purified 7-OH or an uncertain mixture.
Poison centers have received reports of unusual sleepiness, loss of consciousness, slow or difficult breathing, nausea, vomiting, agitation, confusion, sweating, rapid heart rate, high blood pressure, seizures, dependence and withdrawal symptoms. F
The pattern may resemble opioid toxicity in some patients, but mixed or unexpected findings can reflect co-exposures or uncertain product composition.
America’s Poison Centers advises consumers to avoid concentrated 7-OH products and keep them out of the sight and reach of children and pets.
People using products marketed for pain, mood, energy or opioid withdrawal should discuss them with a physician or pharmacist, particularly when they also use prescription medicines, alcohol or other substances.
Anyone who develops unexpected symptoms after taking a 7-OH or kratom-derived product should contact Poison Control in the United States at 1-800-222-1222. Call emergency services if the person is unresponsive, has difficulty breathing, experiences a seizure or cannot be awakened. F
Regular use may lead to physical dependence, and abrupt cessation can produce an opioid-like withdrawal syndrome. Kratom Withdrawal Is Real: What to Expect and What Helps provides additional background on withdrawal and the need for individualised care.
Patients may describe products as “kratom,” “7-OH,” “7-Hydroxy,” “7-HMG,” “7-OHMG” or simply “7.” Clinicians should ask about the exact product, formulation, labelled quantity, source, frequency of use and possible co-exposures.
Assessment and treatment should be guided by the clinical presentation. Sedation, reduced respiratory effort and loss of consciousness should raise concern for opioid-type toxicity. Agitation, seizures, hypertension or mixed findings may indicate co-exposures or an inaccurately labelled product.
Evidence specific to 7-OH poisoning remains limited. Significant respiratory depression, seizures, severe altered mental status or uncertain polysubstance exposure should prompt consultation with a regional poison center or medical toxicologist.
A 2026 retrospective case series described nine patients with problematic purified 7-OH use who began buprenorphine treatment through a telehealth addiction-medicine clinic. Eight were successfully initiated and stabilised, and eight reported improvement at a median follow-up of six weeks. No precipitated withdrawal or adverse events were reported. I
The findings suggest that buprenorphine may help selected patients with clinically significant 7-OH dependence, but they do not establish a standard treatment. The study included only nine patients, had no control group and came from a single service.
The identifiable new developments are the DEA’s 1 July announcement, publication of the formal notices on 6 July, the proposed control of concentrated 7-OH and three related substances, the HHS request for scientific input, the poison-center advisory reporting 901 7-OH exposures during the first half of 2026, and the FDA’s 13 July update.
The pharmacology of 7-OH and the possibility of dependence, withdrawal and respiratory depression are background evidence explaining why the action matters. This story is a new regulatory and surveillance development—not the discovery of a new drug, antidote or proven treatment.
The final threshold, the date of any temporary scheduling order, the number of reports involving verified concentrated 7-OH, the contribution of co-exposures, the highest-risk formulations and the best treatment for 7-OH withdrawal remain uncertain.
The legal status should be checked again when the DEA publishes its next order.
A. U.S. Food and Drug Administration. (2026, July 13). Hiding in plain sight: 7-OH products.
B. U.S. Drug Enforcement Administration. (2026, July 1). DEA to temporarily schedule 7-OH and related substances to protect public safety.
C. U.S. Drug Enforcement Administration. (2026, July 6). Temporary placement of 7-hydroxymitragynine above a specified threshold in Schedule I. Federal Register, 91, 40917–40924.
D. U.S. Drug Enforcement Administration. (2026, July 6). Temporary placement of mitragynine pseudoindoxyl, MGM-15, and MGM-16 in Schedule I. Federal Register, 91, 40909–40916.
E. U.S. Department of Health and Human Services. (2026, July 6). Temporary placement of 7-hydroxymitragynine above a specified threshold in Schedule I: Request for information.
F. America’s Poison Centers. (2026, July 8). Health advisory: Serious illnesses associated with kratom and 7-OH products.
G. Towers, E. B., Thomas, Y. T., Holstege, C. P., & Farah, R. (2026). Increases in kratom-related reports to poison centers—United States, 2015–2025. MMWR, 75, 139–145.
H. Leonard, J. B., Brown, K., & Colvin, J. M. (2026). Kratom exposure cases reported to United States Poison Centers: 2016–July 2025. American Journal of Emergency Medicine, 105, 136–140.
I. Fenske, E., Williams, B. E., Hallock-Koppelman, L., & Buchheit, B. M. (2026). Buprenorphine for the management of 7-hydroxymitragynine use. Journal of Addiction Medicine. Advance online publication.
Regulatory and Policy Updates
Post on 24 Oct 2025

Regulatory and Policy Updates
Post on 30 Oct 2025
Regulatory and Policy Updates
Post on 25 Oct 2025

Regulatory and Policy Updates
Post on 25 Dec 2025
