Body packing and body stuffing are two distinct methods of illicit drug concealment, each posing unique medical, forensic, and legal challenges. Body packers intentionally swallow or insert well-packaged drug parcels for large-scale trafficking, whereas body stuffers hastily ingest or insert poorly wrapped drugs to evade law enforcement. These differing practices influence the risk of toxicity, detection strategies, and management approaches. Diagnostic imaging plays a crucial role in identifying hidden drug packets, with CT scans offering superior sensitivity compared to X-rays. Laboratory investigations, including toxicology screening and metabolic assessments, further aid in evaluating systemic drug absorption and potential complications. Management strategies range from conservative observation and whole bowel irrigation for asymptomatic body packers to aggressive intervention and emergency surgery for symptomatic body stuffers. Drug toxicity management requires rapid stabilization, targeted antidotes, and supportive care. Additionally, legal and ethical considerations present challenges regarding patient confidentiality and law enforcement involvement. Understanding the distinctions between body packers and body stuffers is essential for optimizing medical decision-making, forensic analysis, and legal compliance, ensuring effective patient care and adherence to judicial protocols.
1. Introduction to body packer and stuffer
Illicit drug transportation often involves concealment within the human body, commonly classified as body packing or body stuffing. Body packers engage in drug smuggling by swallowing or inserting drug-filled packets, while body stuffers act impulsively in response to imminent arrest. The implications of these practices differ significantly, necessitating distinct medical management strategies (Heymann-Maier et al., 2017).
2. History and Presentation of body packer and stuffer
Diagnosis starts with suspicion based on the patient’s history, presentation, or law enforcement tip-offs.
Some body packers may be asymptomatic.
Others may present with signs of intestinal obstruction, perforation, or drug toxicity if a packet ruptures.
3. Physical Examination of body packer and stuffer
Examine the patient for signs of drug toxicity, abdominal pain, or obstruction.
Check vital signs for clues about drug effects.
Cocaine can lead to tachycardia, while opioids can cause respiratory depression.
4. Motive of body packer and stuffer
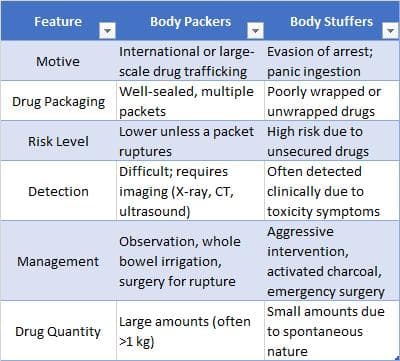
Body Packers: The primary motive is international or large-scale drug trafficking. These individuals often transport well-packaged narcotics across borders to avoid detection (Heymann-Maier et al., 2017).
Body Stuffers: In contrast, body stuffers ingest drugs hastily in response to police intervention, seeking to evade legal consequences rather than to smuggle significant quantities (Aksnes & Jacobsen, 2004).
5. Risk of body packer and stuffer
Body Packers: The risk of acute drug toxicity is relatively lower due to the use of secure packaging. However, in cases of packet rupture, rapid drug absorption can lead to fatal overdose (Heymann-Maier et al., 2017).
Body Stuffers: Due to poorly wrapped or unwrapped drugs, there is a heightened risk of drug toxicity, often necessitating urgent medical intervention (Malbrain et al., 1994).
8. Volume and Quantity of Drugs
Body Packers: Typically carry large amounts of drugs, often exceeding 1 kg, divided into numerous small packets (Shahnazi, 2015).
Body Stuffers: Ingest significantly smaller amounts due to the spontaneous nature of the act (Malbrain et al., 1994).
Understanding the distinctions between body packers and stuffers is crucial for effective medical management and forensic investigation. Body packers engage in premeditated drug trafficking and pose a lower immediate health risk unless the packet ruptures, whereas body stuffers face higher toxicity risks due to insecure drug packaging. Medical and law enforcement personnel must employ appropriate diagnostic and treatment strategies to mitigate potential complications and uphold legal protocols.
Diagnostic Imaging in Detecting Body Packers and Body Stuffers
Detecting concealed illicit drugs within the human body presents a significant challenge for both medical and law enforcement personnel. Individuals attempting to evade detection may swallow or insert drug-filled packets, classified as body packers or body stuffers, based on their intent and packaging. Imaging techniques are critical in identifying these hidden substances and assessing potential complications. This guideline explores the most effective diagnostic modalities and their advantages and limitations.
Body Packers vs. Body Stuffers: Key Differences in Detection
Body Packers: These individuals swallow well-sealed drug packets, making detection challenging. Imaging techniques such as X-ray, CT scan, and ultrasonography are commonly employed (Altuğ et al., 2023).
Body Stuffers: Drugs are often poorly wrapped or unwrapped, making them more susceptible to detection through imaging or clinical signs of toxicity (Heymann-Maier et al., 2017).
Forensic medicine is crucial for legal proceedings to distinguish between body packers and body stuffers. Studies highlight that forensic analysis of human excrements (drug toilets) is a non-invasive yet effective method to confirm drug packet expulsion. However, voluntary defecation control and delayed excretion times may impact results (Mushumba et al., 2021).
Imaging Modalities for Detecting Concealed Drugs
1. Plain Radiography (X-ray)

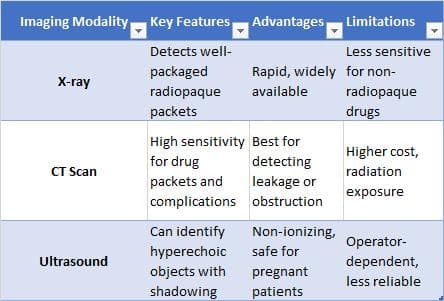
Plain radiography, or X-ray imaging, is the first-line diagnostic tool to detect foreign bodies within the gastrointestinal tract. It is widely available, cost-effective, and relatively quick, making it the most common imaging modality in suspected body packing or stuffing cases.
Key Features: Drug packets appear as oval, well-defined radiopaque densities in the stomach or intestines.
Advantages: Rapid assessment, widely available, and non-invasive.
Limitations: X-ray sensitivity depends on the type of drug packaging. Some packets, especially those wrapped in non-radiopaque materials, may be difficult to detect. While X-ray remains a commonly used imaging modality for suspected body packers, recent studies indicate that CT scans are significantly more sensitive in detecting illicit drug packets and identifying complications such as rupture or obstruction. A five-year retrospective analysis found that 94.4% of drug packets were detected on CT scans, compared to significantly lower detection rates on X-rays (Gheshlaghi et al., 2021).
2. Computed Tomography (CT Scan)
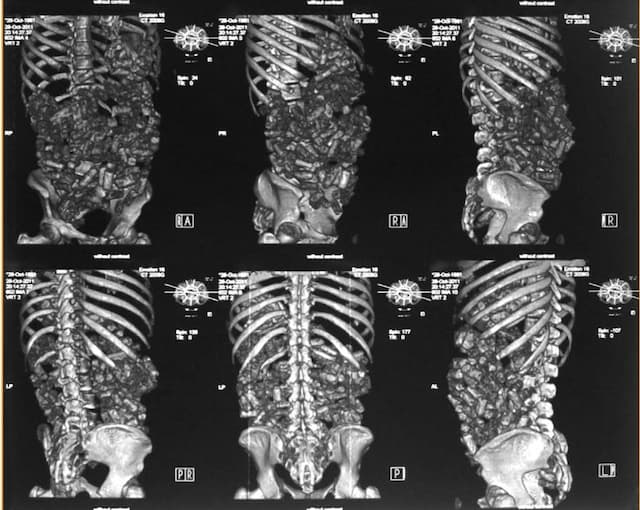
CT scanning is a more sensitive and specific imaging technique than plain radiography, especially when complications such as packet rupture, perforation, or obstruction are suspected. Recent systematic reviews indicate that abdominopelvic CT without contrast is the preferred diagnostic modality for body packers, offering the highest sensitivity in detecting drug packets. Conservative management, including whole bowel irrigation, remains the first-line treatment, but early surgical intervention is necessary in cases of packet rupture or obstruction (Hassanian‐Moghaddam et al., 2019)
Key Features: Detects drug packets with greater clarity, even those missed by X-rays.
Advantages: Higher sensitivity, excellent for detecting leakage of drug contents, gastrointestinal obstruction, and perforation.
Limitations: Higher radiation exposure than X-ray, higher cost, and limited availability in some settings.
3. Ultrasonography (Less Common but Useful in Certain Cases)
While not a primary imaging method, ultrasonography can occasionally aid in detecting drug packets, particularly in resource-limited settings where X-ray or CT scans are unavailable.
Key Features: May reveal hyperechoic (bright) objects with acoustic shadowing in the gastrointestinal tract.
Advantages: Non-ionizing, safe for pregnant patients, and portable.
Limitations: Operator-dependent and less reliable than X-ray or CT scan detecting drug packets.
Diagnostic imaging is pivotal in identifying and managing body packing and stuffing cases. While X-ray remains the first-line tool, CT scans provide superior sensitivity for detecting complications. In special cases, ultrasound can be useful, though its effectiveness is limited. Accurate imaging is essential for timely medical intervention, reducing the risk of drug toxicity, gastrointestinal obstruction, and other severe complications.
Lab Investigations in Detecting and Managing Body Packers and Body Stuffers
Laboratory investigations play a crucial role in diagnosing drug toxicity, monitoring physiological stability, and guiding medical management in cases of suspected body packing or stuffing. While imaging techniques help identify concealed drug packets, lab tests provide essential information on systemic drug absorption, organ function, and potential complications. This guideline explores the key laboratory investigations in evaluating body packers and stuffers.
1. Drug Screening
Drug screening is a vital diagnostic tool when there is suspicion of drug leakage from ruptured packets.
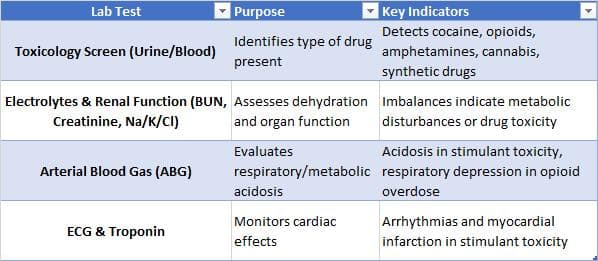
Key Tests: Urine and blood toxicology screens help identify the type and concentration of drugs in the system.
Commonly Detected Substances: Cocaine, heroin, amphetamines, cannabis, opioids, and synthetic drugs.
Limitations: Negative results do not rule out drug packing, as intact packets prevent systemic drug absorption.
2. Electrolytes and Renal Function Tests
Monitoring electrolyte balance and kidney function is essential in patients who may develop dehydration, metabolic imbalances, or organ dysfunction due to drug toxicity or bowel obstruction.
Key Tests:
o Serum electrolytes (sodium, potassium, chloride, bicarbonate): Imbalances may indicate dehydration, acidosis, or alkalosis.
o Blood urea nitrogen (BUN) and creatinine: Assess renal function, especially in patients with dehydration or multi-organ dysfunction.
o Liver function tests (LFTs): Important in hepatotoxic drugs such as acetaminophen-containing substances.
3. Complete Blood Count (CBC)
A CBC provides insight into potential infections, inflammation, or complications such as bowel perforation.
White Blood Cell Count (WBC): Elevated levels may indicate infection or sepsis in cases of gastrointestinal perforation.
Hemoglobin and Hematocrit: Evaluate for anemia or hemorrhagic complications.
Platelet Count: Important for assessing clotting abnormalities, especially if drug-induced thrombocytopenia is suspected.
4. Arterial Blood Gas (ABG) Analysis
ABG testing is useful in critically ill patients to assess oxygenation, acid-base balance, and metabolic disturbances.
Key Indicators:
o Metabolic acidosis: Common in cocaine or amphetamine toxicity.
o Respiratory depression: Seen with opioid overdose, requiring urgent intervention.
5. Cardiac Biomarkers and ECG Monitoring
Drugs like cocaine and amphetamines can cause serious cardiovascular effects, including arrhythmias and myocardial infarction.
ECG (Electrocardiogram): Detects arrhythmias, QT prolongation, and ischemic changes.
Troponin Levels: Elevated troponins may indicate myocardial damage, often due to stimulant-induced vasospasm.
Lab investigations are a cornerstone in managing body packers and body stuffers, particularly when drug toxicity or systemic complications are suspected. Drug screening, electrolyte monitoring, CBC, ABG analysis, and cardiac assessments provide critical insights into patient management. Combined with imaging, these tests help guide clinical decisions and improve patient outcomes.
Management of Body Packers and Body Stuffers: A Clinical Approach
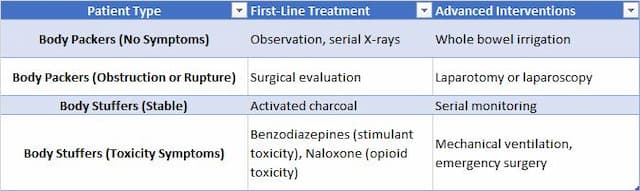
Body Packers: Management includes gastrointestinal decontamination, whole bowel irrigation, and observation. Surgical intervention is considered if packet obstruction or rupture occurs (Wong et al., 2005).
Body Stuffers: Given the higher risk of drug absorption, aggressive intervention such as activated charcoal administration and emergency surgery may be required.
Managing body packers and stuffers requires carefully balancing conservative observation, medical interventions, and surgical procedures. The patient’s symptoms dictate the approach, the integrity of ingested drug packets, and the presence of complications such as toxicity, obstruction, or perforation. This guideline explores the key management strategies employed in clinical settings (Heymann-Maier et al., 2017).
1. Observation for Asymptomatic Patients Asymptomatic body packers with intact drug packets can often be managed conservatively with serial monitoring and imaging (Glovinski et al., 2013).
Key Steps:
o Hospital admission for observation and serial abdominal X-rays every 6–12 hours.
o No food intake to prevent bowel movement acceleration, which may rupture packets.
o Monitor for signs of packet leakage or obstruction, including abdominal pain, vomiting, or altered mental status.
2. Whole Bowel Irrigation (WBI)
Whole Bowel Irrigation (WBI) Whole bowel irrigation (WBI) with polyethylene glycol (PEG) solution is commonly used to expedite drug packet elimination in stable patients (Hassanian‐Moghaddam et al., 2019). WBI can be considered for removal of ingested packets of illicit drugs in "body packers." However, controlled data documenting improved clinical outcomes after WBI is lacking. WBI is contraindicated in patients with bowel obstruction, perforation, or ileus and in patients with hemodynamic instability or compromised unprotected airways. WBI should be used cautiously in debilitated patients and patients with medical conditions that its use might further compromise.
Indications:
Confirmed presence of drug packets with no signs of rupture.
No evidence of bowel obstruction or perforation.
Procedure:
Administer PEG solution via a nasogastric tube at a rate of 1.5–2 L per hour until the rectal effluent is clear.
Continue radiographic monitoring to confirm the complete expulsion of packets.
3. Endoscopic Removal Endoscopic intervention is an alternative for upper gastrointestinal tract packets that are stuck or pose an integrity risk (Wong et al., 2005).
Indications:
o Drug packets lodged in the stomach or esophagus.
o Suspicion of packaging defects that could lead to leakage.
Procedure:
o Gastroscopy is performed to retrieve the packets with minimal risk of rupture.
o Endoscopic removal is avoided if packets have migrated beyond the stomach due to the risk of rupture during retrieval.
4. Surgical Intervention
Emergency surgery is required for cases of packet rupture, gastrointestinal obstruction, or prolonged retention (Yegane et al., 2009).
Indications:
o Clinical signs of acute drug toxicity from packet rupture.
o Evidence of mechanical bowel obstruction that does not resolve with conservative management.
o Retention of drug packets beyond 48–72 hours, indicating possible impaction.
Procedure:
o Laparotomy or laparoscopy is performed to remove the drug packets safely.
o In cases of intestinal perforation, resection and primary anastomosis may be required.
Managing body packers and body stuffers requires a structured approach, prioritizing observation, whole bowel irrigation, endoscopic retrieval, and surgery when necessary. Early recognition and appropriate intervention are critical to preventing fatal drug toxicity and gastrointestinal complications.
Drug Toxicity Management in Body Packers and Body Stuffers
Body packers and body stuffers are at high risk of drug toxicity if the packet ruptures or leaks within the gastrointestinal tract. The severity of toxicity depends on the drug type, dosage, and the rate of systemic absorption. Effective management requires rapid identification of symptoms, administration of specific antidotes, and supportive care to prevent fatal complications. This guideline outlines the essential strategies for managing drug toxicity in these cases (Hassanian‐Moghaddam et al., 2019).
1. General Approach to Drug Toxicity Management
Management is tailored based on the type of drug involved in the rupture.
Immediate stabilization involves securing the airway, breathing, and circulation (ABCs).
Continuous monitoring of vital signs, cardiac function, and neurological status is crucial (Heymann-Maier et al., 2017).
2. Stimulant Toxicity (e.g., Cocaine, Methamphetamine)
Symptoms: Agitation, hypertension, tachycardia, hyperthermia, seizures, and myocardial infarction.
Management:
o Benzodiazepines (e.g., lorazepam, diazepam) to control agitation and seizures.
o Cooling measures for hyperthermia.
o Nitroglycerin or calcium channel blockers for severe hypertension.
o Beta-blockers are generally avoided due to the risk of unopposed alpha stimulation (Kashani & Ruha, 2004).
A recent review of body stuffer cases confirms that benzodiazepines remain the first-line treatment for stimulant toxicity, effectively controlling agitation and seizures. The use of beta-blockers in cocaine toxicity remains controversial due to the risk of unopposed alpha-adrenergic stimulation, and their administration should be carefully considered (Yamamoto et al., 2016).
3. Depressant Toxicity (e.g., Opioids, Heroin)
Symptoms: Respiratory depression, pinpoint pupils, altered mental status, hypotension.
Management:
o Naloxone (opioid antagonist) administered intravenously or intranasally to reverse respiratory depression.
o Mechanical ventilation may be required in severe cases.
o Supportive care, including IV fluids and oxygen therapy (Hassanian‐Moghaddam et al., 2019).
4. Other Drugs and Specific Considerations
Amphetamines: Similar to cocaine toxicity, treated with benzodiazepines and supportive care.
Cannabis: Rarely requires aggressive management; hydration and observation are usually sufficient.
Synthetic Drugs (e.g., MDMA, Bath Salts): Can cause severe agitation, hyperthermia, and serotonin syndrome—managed with sedation, cooling, and cyproheptadine for serotonin syndrome (Heymann-Maier et al., 2017).
5. Supportive Care and Advanced Measures
Airway Protection: Intubation if necessary in comatose patients.
Cardiac Monitoring: Continuous ECG to detect arrhythmias.
IV Fluids and Electrolyte Correction: To maintain hemodynamic stability.
Activated Charcoal (in selective cases): May be administered if there is evidence of early packet rupture and no risk of aspiration (Wong et al., 2005).
The management of drug toxicity in body packers and body stuffers requires a rapid, drug-specific approach to prevent life-threatening complications. Benzodiazepines for stimulants, naloxone for opioids, and aggressive supportive care are the cornerstones of treatment. Close monitoring and timely intervention significantly improve patient outcomes.
Legal and Ethical Considerations in Body Packers and Body Stuffers
Medical professionals must balance their duty of care with legal reporting obligations when treating body packers and stuffers. Patient confidentiality is critical, but in some jurisdictions, healthcare providers are required to report suspected drug trafficking cases to law enforcement if there is a clear legal mandate. However, involuntary disclosure must be weighed against patient rights and ethical principles such as non-maleficence and beneficence.
Reporting Obligations:
o Laws vary by country and state. Some regions have mandatory reporting laws for suspected criminal activities, while others prioritize patient confidentiality.
o Hospitals should follow legal counsel and institutional policies regarding disclosures to law enforcement.
Ethical Dilemmas:
o Reporting a patient may deter individuals from seeking medical attention, increasing morbidity and mortality.
o Physicians must ensure that law enforcement interactions do not interfere with patient care.
o Informed consent should be obtained before engaging with legal authorities whenever possible.
Best Practice Recommendations:
o Healthcare providers should be familiar with local laws on reporting illicit drug activity.
o Clear hospital protocols should outline when and how to involve law enforcement.
o The primary duty is patient safety—clinicians should prioritize stabilization and medical care before considering forensic aspects.
Understanding the distinctions between body packers and stuffers is crucial for effective medical management and forensic investigation. Body packers engage in premeditated drug trafficking and pose a lower immediate health risk unless the packet ruptures, whereas body stuffers face higher toxicity risks due to insecure drug packaging. Medical and law enforcement personnel must employ appropriate diagnostic and treatment strategies to mitigate potential complications and uphold legal protocols, all while considering the ethical and legal implications of reporting suspected drug concealment cases.
References:
Heymann-Maier, L., Trueb, L., Schmidt, S., Carron, P., Hugli, O., Heymann, E., & Yersin, B. (2017). Emergency department management of body packers and body stuffers.. Swiss medical weekly, 147, w14499 . https://doi.org/10.4414/smw.2017.14499.
Malbrain ML, Neels H, Vissers K, Demedts P, Verbraeken H, Daelemans R, Wauters A. A massive, near-fatal cocaine intoxication in a body-stuffer. Case report and review of the literature. Acta Clin Belg. 1994;49(1):12-8. doi: 10.1080/17843286.1994.11718357
Shahnazi M, Hassanian-Moghaddam H, Gachkar L, Ahmadi N, Zamani N, Bahrami-Motlagh H, Faghihi Langroudi T, Arjmand Shabestari A, Mohammad Alizadeh A. Comparison of abdominal computed tomography with and without oral contrast in diagnosis of body packers and body stuffers. Clin Toxicol (Phila). 2015;53(7):596-603. doi: 10.3109/15563650.2015.1054501
Hassanian-Moghaddam H, Amraei F, Zamani N. Management recommendations for body stuffers at emergency units. Arh Hig Rada Toksikol. 2019 Jun 1;70(2):90-96. doi: 10.2478/aiht-2019-70-3199.
Wong, G., Lai, K., & Chung, C. (2005). Management of Body Packers in the Emergency Department. Hong Kong Journal of Emergency Medicine, 12, 112 - 118. https://doi.org/10.1177/102490790501200203.
Glovinski PV, Lauritsen ML, Bay-Nielsen M, Brandstrup B, Bisgaard T. Asymptomatic body packers should be treated conservatively. Dan Med J. 2013 Nov;60(11):A4723.
Yegane, R., Bashashati, M., Hajinasrollah, E., Heidari, K., Salehi, N., & Ahmadi, M. (2009). Surgical Approach to Body Packing. Diseases of the Colon & Rectum, 52, 97-103. https://doi.org/10.1007/DCR.0b013e31819738c9.
Kashani, J., & Ruha, A. (2004). Methamphetamine Toxicity Secondary to Intravaginal Body Stuffing. Journal of Toxicology: Clinical Toxicology, 42, 987 - 989. https://doi.org/10.1081/CLT-200042554.
Yamamoto, T., Malavasi, E., Archer, J., Dargan, P., & Wood, D. (2016). Management of body stuffers presenting to the emergency department. European Journal of Emergency Medicine, 23, 425–429. https://doi.org/10.1097/MEJ.0000000000000277.
Mehrpour O, Sezavar SV. Diagnostic imaging in body packers. Mayo Clin Proc. 2012 Jul;87(7):e53-4. doi: 10.1016/j.mayocp.2012.03.014